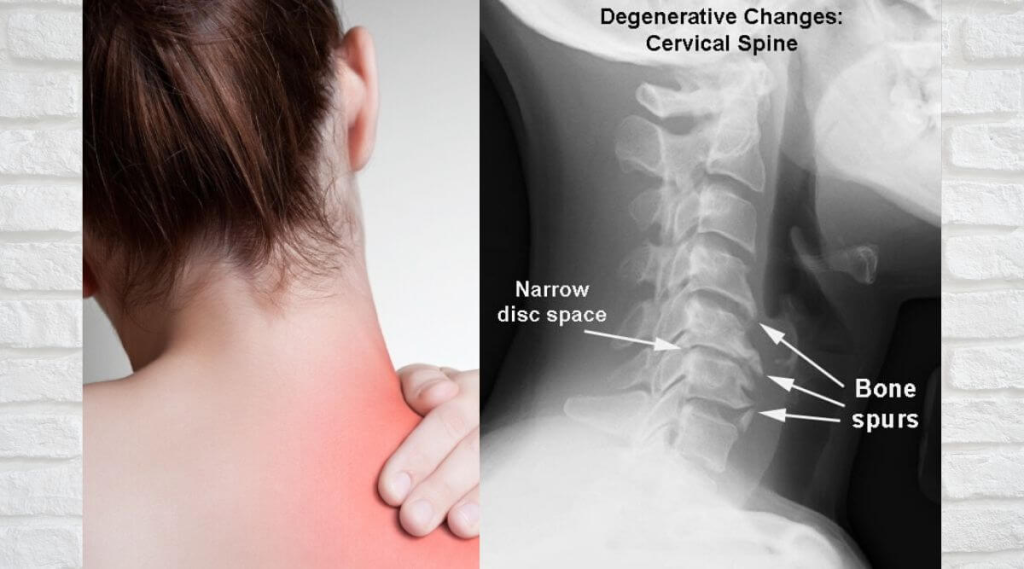
Cervical spondylosis affects 65% of adults by age 50, causing neck pain, radiculopathy, and myelopathy. This degenerative condition requires tailored treatments ranging from conservative care to advanced surgical interventions. Modern strategies emphasize functional restoration and neurological preservation.
Clinical Classification & Diagnostic Workup
1. Subtypes
Type
Characteristics
Diagnostic Clues
Axial Neck Pain
Mechanical pain
Limited ROM, tender facets
Radiculopathy
Arm radiation
Positive Spurling’s test
Myelopathy
Cord compression
Hoffman’s sign, gait disturbance
Vertebrobasilar
Vascular compromise
Dizziness with rotation
Diagnostic Imaging Protocol
X-rays: Dynamic views (flexion/extension)
MRI: Gold standard for neural compression
CT myelogram: When MRI contraindicated
EMG/NCS: Confirm radiculopathy (85% accuracy)
Conservative Treatment Pyramid
Level 1: Acute Phase (0-4 weeks)
Pharmacotherapy:
NSAIDs (celecoxib 200mg BID)
Gabapentin (for radicular symptoms)
Muscle relaxants (short-term use)
Cervical collar: <72 hours to prevent stiffness
Ice/heat therapy: 15min every 2 hours
Level 2: Subacute (4-12 weeks)
Modality
Protocol
Evidence
Manual therapy
Cervical glides (Maitland)
Grade A
Traction
10-15lbs intermittent
Grade B
Dry needling
Trigger point release
Grade B
TENS
80Hz for 20min
Grade C
Level 3: Chronic (>12 weeks)
Therapeutic exercise progression:
Chin tucks → scapular stabilization
Cervical isometrics → resistance training
Ergonomic optimization:
Monitor at eye level (15° downward gaze)
Lumbar-supported sitting posture
Interventional Procedures
Image-Guided Injections
Procedure
Target
Duration
Cervical ESI
Radicular pain
8-12 weeks
Facet RF ablation
Arthrogenic pain
6-12 months
Medial branch block
Diagnostic
N/A
Surgical Indications & Options
Absolute Indications
Progressive myelopathy (mJOA score <12)
Severe radiculopathy refractory to 12 weeks care
Spinal instability (>3.5mm translation)
Surgical Techniques
Approach
Levels
Fusion Rate
ACDF
1-2
95%
Posterior laminectomy
Multilevel
90%
Artificial disc replacement
Single
Preserves motion
Hybrid constructs
Multilevel
Customized
Rehabilitation Protocol
Postoperative Care
Soft collar: 2 weeks (except disc replacement)
ROM exercises: Start at 3 weeks
Strength training: Initiate at 6 weeks
Return to work: Sedentary 4 weeks, labor 12 weeks
Emerging Therapies
Regenerative Medicine
Platelet-rich plasma (PRP): Facet injections
Stem cell therapy: Disc regeneration trials
Neuromodulation
Cervical DRG stimulation: For chronic radiculopathy
VR rehabilitation: Improves compliance
Prevention Strategies
Workstation Ergonomics
30-30 rule: Every 30 minutes, 30sec microbreaks
Voice-to-text software: Reduce flexion
Standing desk: Alternates postural load
Sleep Positioning
Contour pillow: Maintains neutral alignment
Side-lying: With pillow height adjustment
Outcome Measures
NDI: Neck Disability Index
VAS: Pain scale
mJOA: Myelopathy assessment
SF-36: Quality of life
Conclusion
Modern cervical spondylosis management requires risk stratification and multidisciplinary collaboration. While 85% improve with conservative care, timely surgical intervention prevents permanent neurological damage. Emerging biological treatments promise to revolutionize degenerative spine care in the coming decade.